Mouth Breathing
What Every Parent Needs to Know About Mouth Breathing

Have you ever noticed that your child’s lips are parted whenever he/she is sound asleep or playing? If this happens all the time, you should be aware that this is a sign of mouth breathing, instead of nose breathing. It may look cute or funny at first, but the serious health implications behind this behaviour are certainly not.
Our dentists at Paul Dental Clinic will, therefore, discuss the causes and dangers of mouth breathing, and, early intervention.
Normally, we breathe through our noses and this healthy form of breathing produces a range of benefits. The air inhaled through the nose is briefly warmed up, moistened and filtered before it reaches the lungs. Mouth breathing, on the other side, evidently bypasses this process.
What are the causes of mouth breathing?
1. Upper airway obstruction
In order to take in the required amount of oxygen the body needs, the child resolves to breathing through his/her mouth. Often seen in the following cases:
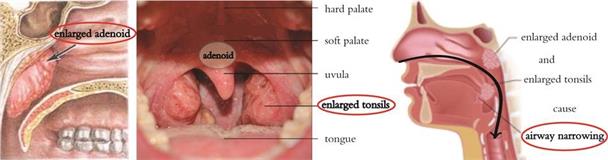
a. Hypertrophied palatine tonsils or adenoids
Tonsils and adenoids are lymphoid tissue located in the pharynx and are the body’s first line of defense, as part of the immune system. It is quite common for them to become infected and eventually excessively swell. Children often have obstructive problems from hypertrophied palatine tonsils or adenoids. The adenoid is located at the very back of the nasal passage; it generally reaches its largest size at 5 years of age and starts to atrophy in late childhood at about 7.
b. Allergic rhinitis
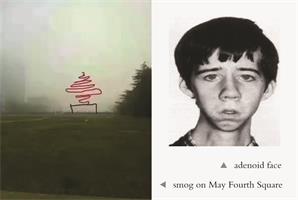
In Qingdao, the occurrence of allergic rhinitis is around 20%, higher than 95% cities in China. The main symptoms of allergic rhinitis are excess nasal secretion, itching, and nasal congestion. Allergic rhinitis is one of the main causes of nasal airway obstruction in young children, and it can interact negatively with adenoid hypertrophy, during which time they are forced to resort to mouth breathing. Persistent mouth breathing may be associated with the development of craniofacial anomalies such as the adenoid facies, as follows. Given the prevalence of smog, parents are advised to specially pay attention to their children’s nasopharynx.
c. Nasal septum deviation, nasal polyps, nasal turbinate hypertrophy and other nasal abnormalities.
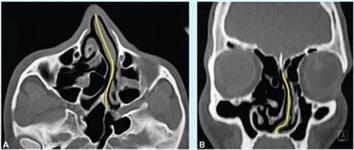
CT shows nasal septum deviation obstructing the airway passage through the nostrils. The main etiological factors of nasal septum deviation are impact trauma, such as a blow to the face.
2. Out of habit
Some children, although can breathe perfectly well through their noses, still choose to breathe through their mouths, out of habit – a bad one indeed.
Habitual mouth breathing can be traced back to breathing issues such as chronic colds, among others, and even if nasal airway is cleared, the habit often still remains.
How does mouth breathing affect the child’s health?
1. Crooked teeth
An important cause of malaligned or crooked teeth is wrong tongue positioning, a common side-effect of mouth breathing.
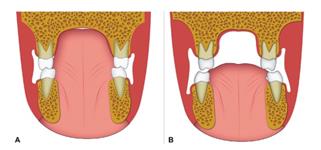
A. Normal tongue position B. Lowered tongue position during mouth breathing
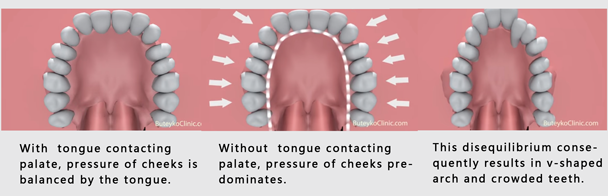
During nasal breathing the tongue rests at the palate and the pressure of the cheeks is balanced by the tongue, which guarantees a normal development of the palate.
To be able to breathe, the mouth-breathing child has to lower his mandible – to keep the mouth open. Since the tongue follows the mandible while resting, it loses contact with the palate. Therefore, inwards pressure from the cheeks is no longer counteracted by outwards pressure from the tongue. This disequilibrium consequently results in the deformation of the upper jaw, creating a v-shaped arch, as opposed to a correct u-shaped arch. The natural development of the upper teeth is disturbed, leading to malaligned or crooked teeth, or even, posterior crossbite.
Meanwhile, during mouth breathing, the tongue may rest against the lower teeth, preventing their normal vertical development, leading to anterior open bite. The association between mouth breathing and open bite is 35.5% in children from 3 to 6 years of age (Gois et al. 2008).

Anterior open bite
2. Periodontal diseases
Chronic mouth breathing is always accompanied with gingivitis of anterior teeth, especially the upper ones. Mouth breathing can quickly dry out the mouth and decrease saliva production. Saliva is very important for neutralising acid and helping to wash away bacteria, without which dental plaque starts to accumulate, causing gingivitis and cavities.

The red, swollen gum of a mouth breather
3. Facial disfigurement
Let’s now have a look at two classic cases of orthodontics on how mouth breathing can adversely affect one’s facial development.
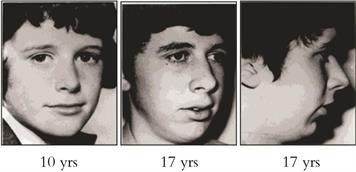
When this boy was 10 years old, he looked great – his lips were together and his face was nicely proportionate. On his 14th birthday, he was given a gerbil as a present, which he kept in his room. Soon after, he developed a severe allergy and because his nose was often clogged, he began breathing through his mouth. Eventually, at age 17, he developed a receded “weak” chin, long face and inconsequential cheekbones.
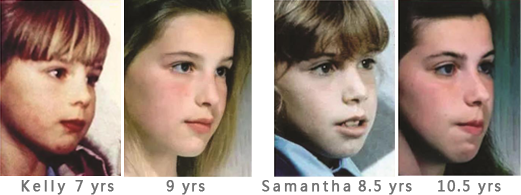
These two sisters, Kelly and Samantha, aged 7 and 8 and a half respectively, visited the dentist because of mouth breathing. They were both taught how to breathe through their noses, and how to swallow correctly, but Samantha did not follow the advice properly. Kelly, on the other hand, took on all what dentist said. 2 years later, we can easily tell that Kelly has the more attractively defined face. The tension on Samantha’s mouth makes her look very unnatural.
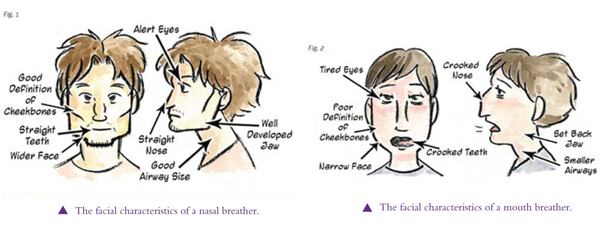
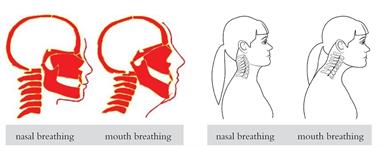
In summary, the comparison of the facial characteristics of nasal and mouth breather are as follows:
Except for the adverse effects on facial development, mouth breathing can also cause forward head posture.
Distally shifted tongue positions result in a further restriction of the airway, and as a result, in order to open up the airway, the neck moves forward and the head tilts backwards. This stresses the spine and fatiques the neck muscles, leading to neck, back and shoulder pain.
4. Other health effects
• Oxygen & sleep
Mouth breathing at night, combined with an obstructed airway, can contribute to low body oxygen content, which may impede the development of important organs. Young mouth breathers often suffer from snoring, or poor quality of sleep, which can cause tiredness and lack of concentration during the day.
• Speech
When children keep an open mouth, they are more likely to struggle with pronunciation.
• Dry lips
• Diminished Sense of Smell
• Breathing Unconditioned Air
Breathing unconditioned air can affect the sensitive tissue of the airway, chance of getting lower respiratory disease increases.
Supplementary Note:
The fact that a child’s lips are often parted is not necessarily a sign of mouth breathing. Given the back of tongue maintains contact with the palate and isolates the mouth, although the lips are visibly separated, no mouth breathing occurs. Whether the tongue presses against the palate or not is the primary deciding factor for complications mentioned above. Thus, the credit of such craniofacial-dental traits in children should not all be attributed to mouth breathing. For example, if a child breathes through his nose, but his tongue never touches his palate, the chances of him/her developing those craniofacial-dental traits are still very high.
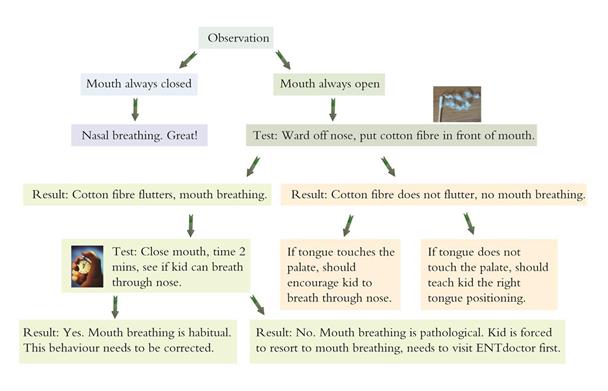
Parents observation chart
Paul Dental Clinic can offer customised appliances to correct behavioural mouth breathing and improve facial myofunction. If your child needs a check-up or consultation, feel free to contact us. We wish that every child has the opportunity to enjoy a good life – with great health and great looks.

• Harari D et al. The effect of mouth breathing versus nasal breathing on dentofacial and craniofacial development in orthodontic patients. Laryngoscope 2010;120(10):2089-93
• Gois, E.G., Ribeiro-Junior, H.C., Vale, M.P., Paiva, S.M., Serra-Negra, J.M., Ramos-Jorge, M.L., and Pordeus, I.A. (2008). Influence of nonnutritive sucking habits, breathing pattern and adenoid size on the development of malocclusion. Angle Orthod, 78, 647–654.
• William R. P. et al. Contemporary Orthodontics 5th edition
• Aravind S. Essentials of Orthodontics